 يحيى الرخاوى طبيب نفسى
يحيى الرخاوى طبيب نفسى
نشرة “الإنسان والتطور”
الأثنين: 18-7-2016
السنة التاسعة
العدد: 3244
الطبنفسى الإيقاعحيوى (73)
Biorhythmic Psychiatry
المقابلة الإكلينيكية (26)
مراجعة سريعة، وتجربة جديدة
إذا كان التشيخص ليس بهذه الدرجة من الأهمية، وكان الإيقاعحيوى دائم النبض بهذه التلقائية، فما هو دور الطبيب النفسى حتى يقوم بمهمته المهنية ودوره الإنسانى وهو يحمل الأمانة ويواصل السعى؟
خطر لى هذا السؤال وأنا أعيد قراءة نشرة أمس فوجب الرد عليه، حتى لو لم أمتلك إجابة كافية.
أولاً: ليس معنى أن الإيقاعحيوى هو نبض دائم طول الوقت ليلا ونهارا أننا ليس لنا دور فى حمل أمانة سلامة نبضه والحفاظ على فطرته وتوجهها كما خلقها مبدعها.
ثانياً: إن الطبنفسى الإيقاعحيوى ليس بديلا عن العلاجات الأخرى ولا هو مجرد مكمّل لها، ولكنه موقف مهنى شخصى واع بضرورة تنمية فن استعمال كل العلاجات الأخرى معا، فهو حين يقدم ضرورة فهم معنى وغائية المرض، ومغزى الأعراض تطوريا قبل الغوص فى الأسباب لا يهمل هذه الأسباب خاصة إذا كانت قابلة للإزالة (الأسباب المديمة الحالية) أو كانت قابلة للتصحيح عبر إعادة بناء علاقات جديدة غير مشوِّهة ولا مشوَّهة.
ثالثاً: إن التعامل مع الكيان البشرى وهو فى “حركة” “إيقاعية” “مستمرة” “متبادلة” طول الوقت، غير التعامل معه وكأنه كمُّ ثابت يقاس بالنقص والزيادة، ثم التصحيح فى المحل.
رابعاً: إن الوعى بحركية الإيقاعحيوى المتبادلة بين شخصين (الطبيب والمريض ابتداء) يعطى للمناقشات اللفظية والاقناع المنطقى والتفسير دورا مساعدا، لا بديلا، ولا استبعاديا.
خامساً: إن تحريك دوائر الوعى الشخصى المتواصلة الاتساع والشمول إلى الوعى البينشخصى إلى وعى الجماعة، إلى وعى الجميع، فالطبيعة فالغيب إلى وجه الحق، كل ذلك يعمل كعامل أساسى فى العلاج يساعد على ضبط تَوجّه الإيقاعحيوى الشخصى مع الإيقاعحيوى الممتد فى الجماعة الأسهل تنغيما وتناغما مع الدوائر الأوسع فالأوسع، ويظهر أثر ذلك أكثر فى العلاج الجمعى وعلاج الوسط، والتأهيل النشاطى الجماعى، جنبا إلى جنب مع وسائل العلاج الأخرى التى تسهم فى نفس الاتجاه وليستّ بديلة عنه.
سادساً: إن فهم الطبيعة البشرية من هذا المنطلق الممتد طولا فى التطور وعرضا فى الطبيعة فالكون: امتدادا إلى المطلق، جدير بأن يغير من محيط وبرامج التنشئة والتدريب على الإبداع النقدى والإنسانى بما يمكن أن يسهم فى حسن التنشئة الطبيعية على مستوى الوقاية بشكل أو بآخر.
وبعد
فأرجو أن أذكّر ما أوصلتنا إليه الفروض المطروحة حتى الآن وهى التى أقدمها كفروض محورية تجمع أغلب ظاهرة ما يسمى المرض النفسى كالتالى:
أولاً: إن كل حركية الحياة هى محاولة لدفع عجلة النمو وإعادة النمو بفضل نبض وتَوجّه الإيقاعحيوى فى اتجاه والإبداع والتطور تفعيلا لبرامج الفطرة كما خلقها بارؤها.
ثانياً: إن كل العصابات هى إما قلق أو دفاعات عكسية بديلة عنه ومحوِّرة له، ونبدأ من الآخر “عن القلق”
ثالثاً: إن كل الأمراض النفسية (عدا العضوية التشريحية) هى دفاعات ضد الفصام بمعنى التوقف والتراجع والسكون والتفسخ فالضمور.
بعد المقدمة:
كلما قلبت فى أوراقى (الآن: حاسوبى) وجدت لى أعمالا ومقالات وفروض هى أقرب ما تكون إلى ما أسميه الآن “الطبنفسى الإيقاعحيوى”، فأتعجب وفى نفس الوقت أطمئن، لأننى أتأكد أن الممارسة هى الأصل، وأن الممارس الجاد حين يسجل خبرته، يسجلها باللغة العلمية الخبراتية [1] التى يتقنها فى وقت وصول الخبرة، ثم قد تتغير اللغة، وتثرى الأبجدية لكن تظل الخبرة هى الخبرة.
لذلك رأيت أن أبادر بإعادة نشر بعض أعمالى الباكرة التى تتناسب مع ما نحن فيه، وأن أترجم بعض ما بها إلى لغة الإيقاعحيوى وأقوم بتحديث البعض الآخر بما يتسير من خبرة جديدة، ومعلومات من قراءات حديثة.
إذا كنت قد قدمت هذا الفرض الأول القائل: إن كل العصابات بما فى ذلك المزمنة والتى صارت طبعا ثابتا، وهى المسماة أيضا “اضطرابات الشخصية” هى: إما القلق، أو دفاعات ضد القلق، فجدير بنا أن نبدأ البحث فيما “هو القلق”، وخاصة أنه لفظ شاع فى الطب النفسى والتحليل النفسى عند العامة والخاصة، ورحنا نتداوله وكأننا نعرفه طولا وعرضا، وشكلا وموضوعا، لكن يبدو أن الأمر ليس كذلك تماما.
من بين أوراقى القديمة التى عثرت عليها اليوم هذا المقال بعنوان:
Anxiety: Structural Orientation
Relation of Conceptualization to Therapy [2]
القلق: من منطور تركيبى
علاقة التنظير بالعلاج
وقد نشر كافتتاحية بالإنجليزية فى المجلة المصرية للطب النفسى فى المجلة المصرية للطب النفسى – العدد الرابع – سنة 1981
وسوف أغامر بنشره كما ظهر حرفيا منذ ثلث قرن دون أية إضافة لعلى بذلك أحقق عدة أهداف هذه بعضها:
أولاً: أن أقدم للزملاء الذين لا يعرفون اللغة العربية (ولا مؤاخذة) فكرى – حتى القديم منه – باللغة الانجليزية لأثبت لهم أننى أستطيع أن أكتب بها، كما جاوت فى هذا المقال القديم، ولكننى مازلت مصرا ألا أكتب بها حاليا.
ثانياً: أن يشتمل ذلك دعوة لبيان علاقة الفكر الذى جاء فيها والذى يظهر من عنوانه أنه فكر تركيبيى Structural ومن منطلق الوعى والدراية، أعنى علاقة ذلك بما أقدمه حاليا مما أسميه الطبنفسى الإيقاعحيوى التطورى.
ثالثاً: أن ألتقط أنفاسى لعلى أستطيع أن أترجم بعض مقتطفات من هذا المقال إذا لزم الأمر ولأربط بينها وبين موضوع القلق من وجهة نظر الفكر التطورى الإيقاعى
4- Anxiety: Structural Orientation
Relation of Conceptualization to Therapy
Introduction
Every word has its particular connotative history. A concept included in a symbol is the result of such history at a particular moment of evolution. Psychiatric vocabulary is the least stable, and in the view of many psychiatrists is of doubtful pragmatic value. The word boundaries in psychiatry (like ego boundaries in schizophrenia) are becoming more ill-defined, let apart the hazards of translation, thus hyper-permeable, in spite of all the efforts given by the members of national and international nosological committees. The concept of anxiety is in no way an exception.
The problem has its direct implications on the how of practice, particularly in terms of therapeutic techniques and goals …etc. The term anxiety provides an additional source of ambiguity since it is originally a lay expression. As Davitz (1969) put it “…the use of such everyday words. adds a considerable potential for confusion in a field that hardly needs additional source of noise in the channels of professional communication”
The available disciplines, placing anxiety as a neurosis, or the mother neurosis, stress two main dimensions viz: a free-floating ill defined fear as well as the autonomic concomitants . Neither could be traced back to the Latin origin where “anxietas” means disquiet while “anger” means constriction. However neither the psychiatric connotations nor the original meaning has adequate correlation with the differential therapeutic orientation.
As a developing country as we are, we are not (or should not be) the least satisfied by reproducing the imported, sometimes illusive, information about the subject. We have to search before all for the useful meaning. As Kendell (1975) puts it “.it is almost meaningless to ask which is right. The appropriate question is always which is more useful or appropriate and the answer varies with the purpose in mind” I hope or believe that our purpose in mind is primarily therapy and not the least stereotyped pseudo-communication.
Concepts and Practice
A concept in psychiatry is, or should be, primarily derived from feedback in clinical practice. It should be understood as a logical phenomenological approach through an evolutionary psychopathological orientation where psychopathology is neither etiology nor symptomatology but the psycho structural morbid organization along more than one axis and dimension. Both conceptualization and practice are directly influenced by the personal defenses of the psychiatrist as well as the attitudes and values imposed upon him from society as a spatio-temporo-environmental incidence.
1- Anxiety for a therapist who conceptualized health as the “anxiety free nirvana” would differ from another believing in life as a crescendo dialectic synthetic formation always in the make.
2- Understanding anxiety as a ” language for” rather than “a manifestation of “or” resulting from“: that is to say adding teleology to determinism is apt to alter the therapist’s stand and to favour certain therapeutic procedures.
3- Interpreting the presenting “form” of anxiety in terms of behavioral manifestation of some morbid organization (personality organization as well as neuronal and molecular) varies from interpreting it in terms of some manifestations of this or that brain amine or in terms of a mal-learning or residual fixation.
The Suggested Approach:
The syndrome, or symptom, called anxiety could be conceived through multitude of aspects:
- i) on behavioural level as a symptom or syndrome refers to that ill-defined fear associated with autonomic manifestations.
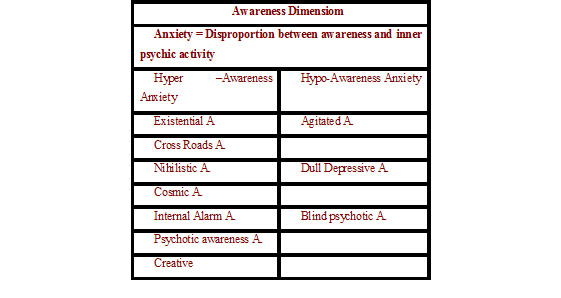
- ii) on behavioural On a deeper level related to awareness, anxiety is to be considered as a phenomenon of hyper-arousal resulting from a disproportion between the scope of awareness and the intrapsychic activity.
iii) On psychostructural level, anxiety could present in different forms according to the underlying structural formulation.
I- Awareness Dimension
The hyper-arousal awareness referred to just now is essentially relative. It refers to the discrepancy between the intrapsychic activation (with or without external objective stirring up forces) and the coping of the holistic awareness with such activation terms of. If the hyper-arousal is due to hyper-awareness more subjective symptoms and less autonomic and motor symptoms are met with. The contrary occurs in cases of hypo-awareness arousal i.e. more irritability and autonomic manifestations are met with.
1) Hyper-awareness anxiety
In general this refers to a state of relative increased dose of awareness which could be met with in healthy growth crises, in creative experience as well as various morbid states of handicapping hyper awareness. In this special presentation I shall not delineate the healthy from the pathological as it is, in most cases, a matter of dose and handical as manifested in the tolerance and outcome. It should be differentiated from intellectual tual insight in the morbid inner life which could be only part of the syndrome to alleviate some of the internal objective confrontation.
The overlap between subcategories of this group is much more met with, The specific term of a sub-type only refers to the dominant characteristic feature .
a-Existential anxiety
This is a recently applied term in psychiatry borrowed from philosophical vocabulary. It refers to a certain degree of awareness of on”s true self e.g.in boundary experience (K. Jaspers) or of the absurdity and meaninglessness of the world as such (J.P.Sartre). It is neither healthy or unhealthy in itself. Under appropriate conditions it should be an intermediate stage the further specification of which is related to the outcome. As such, it could be also called Cross-Roads anxiety particularly when choice and re-choice is emphasized.
Cross-roads anxiety:
This term has been used by the author (Rakhawy 1979) to refer to the cross roads crises declaring the peak of a growth experience where the old organization fails while the new one has not yet been sufficiently established to be put into action as a dominant or leading. When anxiety predominates such crises the suggested term is justified. In the original publication it has been cited as independent subtype but I preferred to make it as basic for most other categories in this main hyperawareness group. It is characterized by deeper reorientation in one”s self and in the reality around (usually associated with or ushered by depersonalization and derealization). By definition it could take any road (hence outcome) according to different variables (personal predisposition or environmental factors) Most hyperawareness types are cross roads experiences but levels differ. While it is related to free choice in existential anxiety it is more related to nihilism in nihilistic one. Also cosmic anxiety is cross roads one between mystical experience, regression and mania. Psychotic awareness anxiety is also a declaration of cross roads impasse that could lead to any psychotic presentation particularly disorganization.
c-Nihilistic anxiety
This type is usually considered as a variant of existential anxiety but with selective hyper-awareness related to the futility of life (e.g.Camus).The overdose of awareness uncovers the aimless, doubted finality of one”s existence. Depression or nihilistic schizoid withdrawal may be met with from the start or may ultimately supervene. Here the selective hyper-awareness is usually related to the limited existence span of the individual and not infrequently projected onto others.
d-Cosmic (&Mystic) anxiety:
When hyper-awareness extends beyond one”s own existence (as a mesa-cosmos) to surpass his limited personal time and space, one may be confronted with cosmic orientation (macro-cosmos) beyond his ability to assimilate such experience at once. This may continue in either way, either to establish a higher level of relatedness and harmony beyond one’s own personal existence and thus elaborates a specific growth experience or, otherwise, it may start some other morbid march towards manic detachment or still worse disorganizing outcome. As such it is a cross roads variant as well.
e-Internal alarm (phobic) anxiety:
This is usually described under phobic disorders in terms of fear of insanity, fear of loss of control, or any other fear from some activated intrapsychic structures.(E.g. from being helpless once again , from some homicidal impulse or from incestuous inclinations, etc..).It is not fair to put such fears as simple phobias since they declare directly the result of hyper-awareness in what is actually present inside everybody. Such awareness could be related to uncovering (or impending uncovering) of deeper intrapsychic reactivated ontogenetic or phylogenic structure. The so called psychotic ego is perceived as an active impending hostile monster rather than a negative inert outcome of some breakdown of the previously existing organization.
It is claimed that such phobias are usually concomitant with depression. This is partly true but its structural interpretation still refers to hyper-awareness in one’s intrapsychic content and the depression could be the result of excessive control in a trial to compensate for such dangerous awareness.
f-Psychotic awareness anxiety:
In the early stages of a psychotic process, the patient is occasionally submitted to sudden uncovering of the intrapsychic content which presents directly in the overt conscious matrix as a real overwhelming bare unusual existence, not only feared of, acted out or alienated.
This phenomenon has been described by the author as awareness of the psychotic or psychotic awareness (Rakhawy 1979) in contrast with psychotic insight of Arieti (1974). It is less dynamically manipulated as in case of internal alarm anxiety. It declares actual activation rather than impending one or fear of outcome. This direct perception of the seves and reality as “they are” is usually associated with real apprehension, astonishment, fluctuating perplexity, depersonalization experience and occasional suspicion. Not infrequently, ixed forms are met with declaring both hyper-arousal and hypo-awareness at a time. The outcome of such stage of instability is usually more serious than the previous ones since the dose of activation and direct uncontrolled confrontation are definitely higher than any possibility for assimilation..
g-Creative anxiety
Such type characterizes the prodromal or the preparatory stages of creative experience. Basically it could not be differentiated from existential, cosmic or even psychotic awareness. Nihilistic anxiety in the process of creation is more related to the fruitlessness of the older organization. The creative outcome either as a creative product or creating ones”self determines its categorization here and not elsewhere under a pathological label. Diagnosis is made, then in most case, in retrograde.
1-Hypo-awareness anxiety
The anxiety in this variant manifests predominantly as motor and autonomic hyper-arousal.The disproportion between a restricted awareness in the face of an unduly activated intrapsychic structure is responsible for this type. I am not going to give new examples to illustrate this type since they constitute the main bulk of anxiety syndromes as described behaviourally. However, tension anxiety, exhaustion anxiety (neurasthenia), agitation anxiety and projected phobic anxiety could be included here. When the psychotic awareness anxiety is associated with hypoawareness rather than hyperawareness it could be overwhelmingly disorganizing.
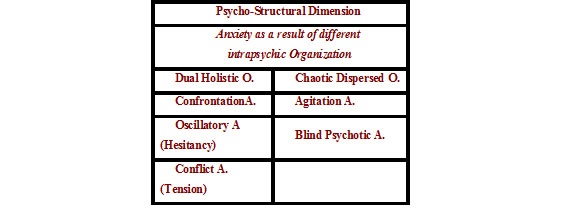
II-The Structural-Organization Dimension
The second dimension which could clarify our conceptualization of anxiety particularly in relation to therapy is the how of organization of the personality structure where any outcome is simply the outer facade of such organization. This dimension is the most difficult to assess but again it is perhaps indispensable to uncover. It is directly related to the psychiatrist”s theoretical orientation about the how of organization of the personality and of the brain.
Different presentations of anxiety according to the how the multi-organizations (assumed or real intrapsychic wholes or persons ego states etc..) are inter-related is tried in this section.
If the personality is still preserving certain whole organizations, mainly two outstanding (dual), some coherent presentation could be described and grasped. On the contrary the personality could no more represent such wholes but rather an agitated chaos and in this case other types of anxiety could be met with. With the risk of reductionism two main categories are introduced: The dual holistic one and the chaotic one.
A– Dual Holistic Organization (type) This main category comprises the following types:
1-Confrontation Anxiety
When two main organizations (say : old- new, child-parent , social-native or right-left hemispheres… Etc.) Confront each other for dominance while both are equally strong some behavioral manifestations are presented declaring this equivalence. Depression is the main result of such structural pattern but occasionally a special form of anxiety dominates the clinical picture usually along with the depressive symptoms. Phobias which are respondent to anti-depressive therapy could be variants of this type.
2-Hesitancy (Oscillatory) anxiety
Instead of confronting each other, simultaneously reactivated structural organizations may oscillate alternating rapidly with one another presenting symptomatically as hesitancy, unsustained activity, occasionally lability and ambivalence. Such type is mainly met wit in early disorganizing psychoses sometimes called acute schizophrenia, in extremely rapid cycling manic depressive syndrome, in borderline
personality (of DSM III) as examples. They are not called anxiety in its final presentation as symptoms. However the stirred-up shifting disorganization worth considering as anxiety from a structural point of view.
3- Conflict (tension) anxiety:
The word conflict is usually used in psychiatry to declare the dynamic relation of any opposing forces. In this context it is indicative that one structural organization has achieved some relative dominance over the other while the latter does not yield totally, still performing its active traction and influence, although at a distance (less confronting). This assumed distance differentiates this type from confrontation anxiety. . Behaviourally this type is manifested as a symptom mainly in the form of tension and exhaustion.
B-The Chaotic Organization
This type is occasionally known as psychotic anxiety and less frequently as disorganization anxiety. It could be arbitrary classified into two main variants. The chaotic dispersed, and the the blind agitated.
1-Chaotic Dispersed anxiety
One can identify here the dispersion of energy as a result of multiple organizations losing their own unity. Perhaps this is mainly manifested in schizophrenic anxiety and in the course of organic dementia (crise de perplexite of Henry Ey). It is characterized by vagueness, hesitancy, fluctuation and hyperkinetic agitation. It could be also met with in some akasthesias resulting from prolonged use of major tranquilizers. Such complication could be interpreted in terms of irregular displacement of energy through loosely associated fragments of organizations.
2-Blind agitated anxiety
This other type is also called psychotic anxiety. It has been referred to it in relation to psychotic awareness anxiety, where the sever haphazard activation is associated with hypoawareness. The result is restricted consciousness associated with extreme emotional turmoil with its motor and autonomic accompaniments.
Rationale and clinical utility of the approach :
It is evident that the word anxiety here has included more than it should. This introduction did mean to replace the included symptoms under the one omnipotent over-inclusive word. It is a trial to go back to the origin of psychic disharmony and to present psychiatric phenomenon through more holistic approach.
In practice this apparent difficult (or rather splitting approach) could be directly related to the how of management more than the definition of a psychiatric symptom by other words can do.
The goal of therapy is to restore, once again, a functioning balance between the dose of awareness and the ability to assimilate its consequences as well as to control the surplus intrapsychic activity. This could be established first through adjusting the dose of awareness, the ability to assimilate the activated intrapsychic structure and proper timing. Such approach for identifying and understanding anxiety on one hand in relation to awareness and on the other hand from an organizational point of view could be very helpful to consider in the therapeutic planning.Of course it needs special training and definite artistic healing approach which is but medicine.
Conclusions
As Tyrer (1979) put it “..The recognition of anxiety in a psychiatric patient is but the first step in classification..” . it is more logic that the same principle applies to therapeutic planning. Answering the following questions may help to clarify one”s concept about a particular case and consequently the nature of possible therapy to be applied:
1-Is anxiety in a given person, a direct declaration of an overdose of awareness or is it a defense against impending untimely dose (of awareness) ?
2-What is the underlying morbid (not only premorbid) structural organization?
3-How is it (anxiety) presenting? Predominantly behavioral autonomic acting out with consequent perception of the bodily alterations or is it perceived more as a phenomenon related to consciousness and subjective experience?
4-What does anxiety mean for this particular person, in this particular presentation, in this particular time at this particular stage of evolution and in that particular society?
5-What are the resources of such person to cope with such morbid situation? Will he be able to assimilate more of the activated structure or is he obliged to suppress whatever is intolerable and narrow more and more his scope of awareness (the same applies to the therapist depending on who is he and to what is he after.
References
Arieti,S.(1974) Interpretation of Schizophrenia. New York: Basic Books.
Davitz,J.R.(1969) The Language of Emotion. New York: Academic Press.
Ey, H.(1950) Etude Psychiatrique. Tome II, Paris: Desclee de Brouwer et Cie.
Kendell, R.E.(1975) The role of diagnosis in Psychiatry Oxford: Blackwell Scientific Publications.
Rakhawy, Y.(1979) A Study in Psychopathology. Cairo: Dar El Ghadd. In Arabic.
Tyrer,P.(1979) Anxiety States. In Granville-Grossman, K. (Ed) Recent Advances in Clinical Psychiatry, 3rd ed. London: Churchill and Livingstone.